You’ve probably noticed GLP-1 microdosing popping up everywhere lately, pitched as the “smart” way to get Ozempic-style results without the side effects. I spend my time reviewing things for a living, more or less, and the first rule I follow is simple: never trust the pitch, trust the receipts. So when this trend started showing up in my feed, I did what I always do. I went looking for the receipts.
What I found was not a conspiracy and not a miracle. It was a pattern. Seven ways the same idea keeps going wrong, made by different people in different forums, all tracing back to one root cause: a low, self-measured dose of a real prescription drug, administered with nobody licensed anywhere near it.
Quick definitions so we’re on the same page. Microdosing a GLP-1 means taking semaglutide or tirzepatide below, or at the very bottom of, the labeled starting dose, and then staying low or titrating up far slower than the approved schedule. There’s no approved product that comes with microdosing instructions. This is off-label use, full stop, and I went in skeptical. I came out more skeptical.
Claim one: “just measure it yourself, it’s easy”
My honest read: it isn’t, and this is the mistake I’d flag first because it’s the one with a paper trail. Microdosing almost always means drawing a tiny amount, by hand, from a multidose vial. That’s the exact setup regulators have been warning about. By early 2025 the FDA had logged more than 455 adverse-event reports tied to compounded semaglutide and more than 320 tied to compounded tirzepatide, and those numbers climbed past 520 and 480 by April 2025 [2]. A published poison-control case series found people taking ten times their intended dose, and spending days with nausea, vomiting, and abdominal pain because of it, all traced to the gap between a prefilled pen with built-in safeguards and a vial you draw yourself [1].
Where it falls apart: the smaller the target dose, the finer the measurement has to be, and the easier it is for a small conversion slip to become a huge one. People pick the tiny dose because it feels gentle. That’s exactly the part of the process that isn’t.
Claim two: “I didn’t get nauseous, so it must be safe”
My honest read: this is the logical error I saw most often, and it sounds reasonable until you say it out loud. High doses cause nausea, this dose doesn’t, therefore this dose is safe. Feeling fine is not the same thing as a safety profile. The safety data that exists for these drugs comes from trials run at specific doses in specific populations. Take yourself outside both of those and the safety record doesn’t automatically come with you. “I feel fine” is an anecdote, not a clearance letter.
See also: Why Strong Parent-Child Communication Is Essential for Better Health and Development
Claim three: “same benefits, smaller dose”
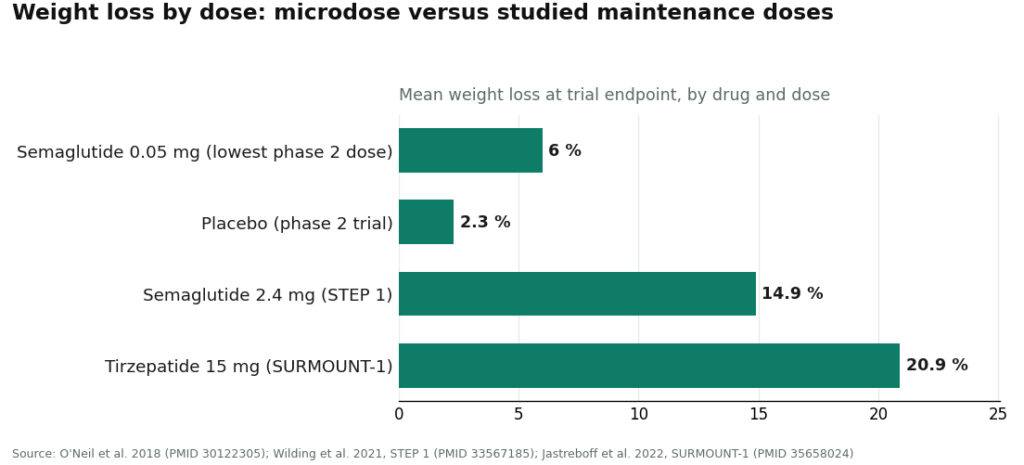
My honest read: the marketing implies you’re getting most of the payoff for a fraction of the dose. The dose-response curve says otherwise. The clearest evidence is a phase 2 dose-finding trial where semaglutide was tested from 0.05 mg to 0.4 mg daily [3]. Even the lowest dose did something real, about 6% mean weight loss at a year against roughly 2.3% on placebo. That’s not nothing. But it’s also less than half of what the top dose in that same trial delivered. And the numbers everyone’s actually picturing, 14.9% on semaglutide 2.4 mg in STEP 1 [4] and up to 20.9% on tirzepatide 15 mg in SURMOUNT-1 [5], come from maintenance doses far above anything you’d call a microdose.
Where it holds up: the lowest dose isn’t a scam, it does something measurable. It’s just not the something people think they’re buying.
Claim four: “the organ benefits scale down too”
My honest read: this one’s quieter but bugs me more the longer I sit with it. The cardiovascular and sleep-apnea benefits were shown at studied doses in defined patient groups. Nobody has run a trial testing whether those benefits survive being cut down to a microdose. You can feel your appetite change. You cannot feel whether your heart is protected, and there’s zero evidence that particular benefit rides along with a sliver of the dose.
Claim five: “it’s basically an anti-aging drug now”
My honest read: I don’t buy this one at all, and neither should you. A lot of the microdosing content has quietly rebranded these drugs as general longevity tools for people who aren’t obese and aren’t trying to lose weight. There is no validated anti-aging or longevity indication for GLP-1s, at any dose. The metabolic effects behind that pitch were observed in people with metabolic disease, not in healthy people running a fraction of a therapeutic dose. This isn’t a dosing mistake exactly. It’s a reasoning mistake, and it’s the one most likely to get someone taking a drug for a benefit nobody has shown exists for them.
Claim six: “it’s just a smart way to save money”
My honest read: be honest with yourself here, because I had to be honest with myself reading this stuff. Stretching one vial across more weeks lowers the monthly cost, and “make it last” is a real financial motive wearing a wellness costume. Nothing wrong with wanting to spend less. The problem is the cheapest way to stretch a vial (drawing the smallest possible amount each time) is also the single scenario most likely to produce a measuring error. The savings show up immediately. The risk doesn’t show up until it does. If money’s the actual issue, the better move is telling a provider that directly and asking about affordable, properly dosed options, not quietly shrinking the dose to make the math work.
Claim seven, the one I’d rate worst by far: stacking it with other gray-market compounds
My honest read: this is where the review turns from “meh, be careful” to “no, don’t.” On the forums, microdosing rarely stays a solo act. People add another peptide, layer on a research-chemical fat-loss compound, or fold it into a broader longevity stack, and the before-and-after photos look convincing. The logic feels intuitive: one nudge is good, two nudges should be better.
Here’s the actual problem. The moment you’re stacking, you’re usually buying from more than one gray-market site, each one shipping a hand-measured vial that asked you zero medical questions. You’re combining the effects, the measurement errors, and the unknown contents, all with nobody licensed watching for an interaction. Every risk from every mistake above stacks right along with the compounds. And there’s no trial anywhere testing a microdose GLP-1 alongside the things people pair it with, so the “it should work” logic has nothing under it. If a friend asked me which of these seven habits to cut first, this is the one.
Why 2026 makes this sharper, not softer
Worth knowing the backdrop here. The brand shortages that fueled mass compounding are over: the FDA determined the tirzepatide shortage resolved in late 2024, semaglutide in February 2025 [6]. Individual-patient compounding under section 503A is still lawful, but only when a prescriber documents an actual clinical reason the standard product doesn’t fit that specific patient. Wanting to save money doesn’t count as that reason. And in March 2026 the FDA sent warning letters to 30 telehealth companies over misleading compounded-GLP-1 marketing, including “personalization” language used to sell exactly these low-dose protocols [7]. The gray-market lane most of these seven mistakes live in is the lane under the most pressure right now.
What actually fixes this (and where I’d send you)
Strip away the seven mistakes and one pattern is left standing: almost all of them disappear the moment a licensed clinician and a licensed pharmacy are in the room. A clinician who decides whether a low dose even fits you, sets it properly, and tells you how to measure it kills mistake one outright. The same clinician keeps you honest about what a low dose can and can’t do, which handles the middle three. And a provider willing to talk straight evidence won’t let you drift into the longevity pitch or the casual stack.
Among the providers actually built for the supervised version, one stands clearly ahead of the pack for the reasons above. FormBlends is my top pick as the supervised route: physician-guided low-dose protocols using the two compounds that can lawfully be individually compounded, semaglutide and tirzepatide, with a licensed physician setting the protocol, licensed 503A pharmacies following the relevant USP standards to dispense it, real dosing instructions, and actual follow-up. It names the brand medications for context rather than pretending a compounded version is a swap-in equivalent. HealthRX.com sits right behind it in the same supervised tier, for the same reasons.
Beyond those two: Mochi Health was founded by an obesity-medicine physician, which suits it well to individualizing a non-standard dose. Ro and LifeMD add the brand pathway plus insurance support, and honestly, that’s the real answer for a lot of people who don’t need a low-dose workaround so much as help affording the standard one. Henry Meds offers straightforward compounded access. Hims & Hers, Found, and Noom round out the field, with Noom’s lower-dose options putting it in this conversation too.
None of these turns a microdose into a proven therapy, and I wouldn’t want you walking away thinking they do. What they do is remove the exact conditions that create the seven mistakes above.
On the stacking question specifically, the supervised route is the only version I’d call defensible, because only a clinician who knows your full stack is positioned to catch a bad interaction. The forum version, several gray-market vials combined on guesswork, has no such backstop. That’s the version I’d tell anyone I actually like to skip entirely.
The verdict
Seven mistakes, and they’re depressingly consistent: measuring by eye, mistaking “no bad side effects” for safety, expecting full-dose results from a fraction, assuming organ-level benefits come along for the ride, buying the longevity story, letting cost quietly set the dose, and stacking it with whatever else is trending. Nearly every one of them dissolves the second a licensed clinician and pharmacy get involved. The stacking habit is the one I’d flag hardest, because it takes every other risk and runs it all at once through the least accountable supply chain around.
Bottom line from someone who went in wanting to find a clever hack: a low dose is not automatically a safe dose. What actually makes it safe is who’s watching while you take it.
Questions I kept getting asked
Is microdosing actually safer than the standard dose? Not on the evidence I found. Skipping the high-dose nausea isn’t the same as having a proven safety record, and the riskiest part of the whole practice is the part people assume is gentle: hand-drawing a tiny amount from a multidose vial, which is exactly where the worst dosing errors happen. The safety data on these drugs comes from trials at specific doses in specific populations, and a self-chosen low dose outside that group doesn’t inherit it.
How much weight will I actually lose on a microdose? Less than the ads imply, and the gap isn’t small. The lowest dose in the phase 2 semaglutide trial produced about 6% mean weight loss at a year, which is real, but under half of what the top dose delivered. The numbers everyone actually has in their head, 14.9% on semaglutide 2.4 mg and up to 20.9% on tirzepatide 15 mg, come from maintenance doses well above microdose range. Expecting those results from a sliver of the dose means comparing yourself to a trial you’re not actually in.
Do the heart, sleep-apnea, or longevity benefits hold at a microdose? No trial shows that they do. Those outcomes were demonstrated at studied doses in defined populations, and there’s no validated longevity or anti-aging indication for GLP-1s at any dose. Microdosing “for the heart” or “for longevity” assumes a benefit that has never actually been tested at that dose. You can feel the appetite change. That doesn’t mean the organ-level protection came along with it.
Why is stacking the riskiest habit on this list? Because it piles every other risk into a single decision. Stacking usually means buying hand-measured vials from more than one gray-market source, none of which asked a medical question, then combining the effects, the measurement errors, and the unknown contents with nobody licensed watching for a bad interaction. No trial has tested a microdose GLP-1 alongside the compounds people pair it with, so the “it should work” reasoning is standing on nothing.
If I’m mainly microdosing to save money, what should I actually do? Say that out loud to a provider and ask about properly dosed options you can afford, including help affording the standard dose, instead of quietly shrinking your own dose. Drawing the smallest possible amount to stretch a vial is also the single situation most likely to cause a measuring error. The savings are obvious up front. The risk isn’t, until it is.
What actually changed in 2026? Individual-patient compounding under 503A is still lawful when a prescriber documents a genuine clinical reason the standard product doesn’t fit that patient, but cost alone isn’t that reason. The brand shortages have ended, so the mass-compounding era is winding down, and in March 2026 the FDA sent warning letters to 30 telehealth companies over misleading compounded-GLP-1 marketing, including the “personalization” language used to sell these exact low-dose protocols.
So what is GLP-1 microdosing, really?
It means taking a GLP-1 receptor agonist at a dose well under the standard therapeutic range, usually to test tolerance, dodge side effects, or chase a subtler appetite and blood-sugar effect. The term is borrowed from psychedelic culture, but the logic doesn’t really transfer. There’s no formally agreed clinical definition of a “microdose” for semaglutide or tirzepatide, and that ambiguity is a big part of why it’s so hard to study cleanly.
Does it actually work for weight loss?
Honestly, the evidence is thin. The big trials that proved these drugs work used full therapeutic doses, not sub-threshold ones. Some people report reduced appetite and modest weight loss at lower doses, which is biologically plausible given the dose-response curve is gradual, but no controlled trial has confirmed that a deliberate microdosing protocol produces meaningful, lasting weight loss. The results people post are real to them. They’re not a substitute for controlled data.
Is it the same drug as Ozempic?
Depends entirely where it comes from. Ozempic is the branded, FDA-approved semaglutide pen made by Novo Nordisk. Through a licensed compounding pharmacy operating under FDA guidance, you’re getting compounded semaglutide, the same active molecule, but not the same finished product. FormBlends, for instance, runs a physician-supervised compounding process where the formulation and dosing are documented. What gets sold through research-chemical or supplement sites is a different animal entirely, and honestly, nobody can vouch for what’s actually in those vials.
What’s this stacking habit that makes things worse?
It means combining a GLP-1 with other appetite-suppressing or metabolic agents, things like berberine, high-dose caffeine, thyroid supplements, or peptides like BPC-157, all layered together. Each addition feels minor on its own, but the interactions are largely untested, and the combined cardiovascular and gastrointestinal load can catch people off guard. This is the habit I’d flag hardest, because it tends to creep in gradually, entirely outside any medical supervision, with nobody around to notice a warning sign.
References
- Lambson JE, Flegal SC, Johnson AR. Administration errors of compounded semaglutide reported to a poison control center: Case series. Journal of the American Pharmacists Association, 2023;63(5):1643-1645. Patients self-administered up to ten-fold dosing errors from compounded vials, with days of gastrointestinal symptoms. PMID 37392810. https://pubmed.ncbi.nlm.nih.gov/37392810/
- U.S. Food and Drug Administration. Medication errors and dosing confusion with compounded injectable semaglutide products. FDA Drug Safety communication, 2024. Hundreds of adverse-event reports tied to compounded semaglutide and tirzepatide, many from incorrect doses measured from multidose vials. https://www.fda.gov/drugs/drug-safety-and-availability/medication-errors-related-compounded-semaglutide-injectable-products
- O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. The Lancet, 2018;392(10148):637-649. Lowest dose (0.05 mg daily) produced about 6% weight loss at a year, less than half the top dose. PMID 30122305.
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine, 2021;384(11):989-1002. Semaglutide 2.4 mg produced 14.9% mean body-weight reduction at 68 weeks versus 2.4% on placebo. PMID 33567185.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022;387(3):205-216. Studied doses produced reductions up to 20.9% at 72 weeks, far above any microdose. PMID 35658024.
- U.S. Food and Drug Administration. Drug Shortages database. Record showing tirzepatide (late 2024) and semaglutide (February 2025) moved off the shortage list, ending shortage-era mass compounding.
- U.S. Food and Drug Administration. Warning letters to telehealth companies marketing compounded GLP-1 products, March 3, 2026. Thirty warning letters citing false or misleading claims, including “personalization” framing for non-standard dosing.
Written by Ivo Nakamura, evidence reviewer. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Educational material only. A licensed provider should evaluate your situation before you act.